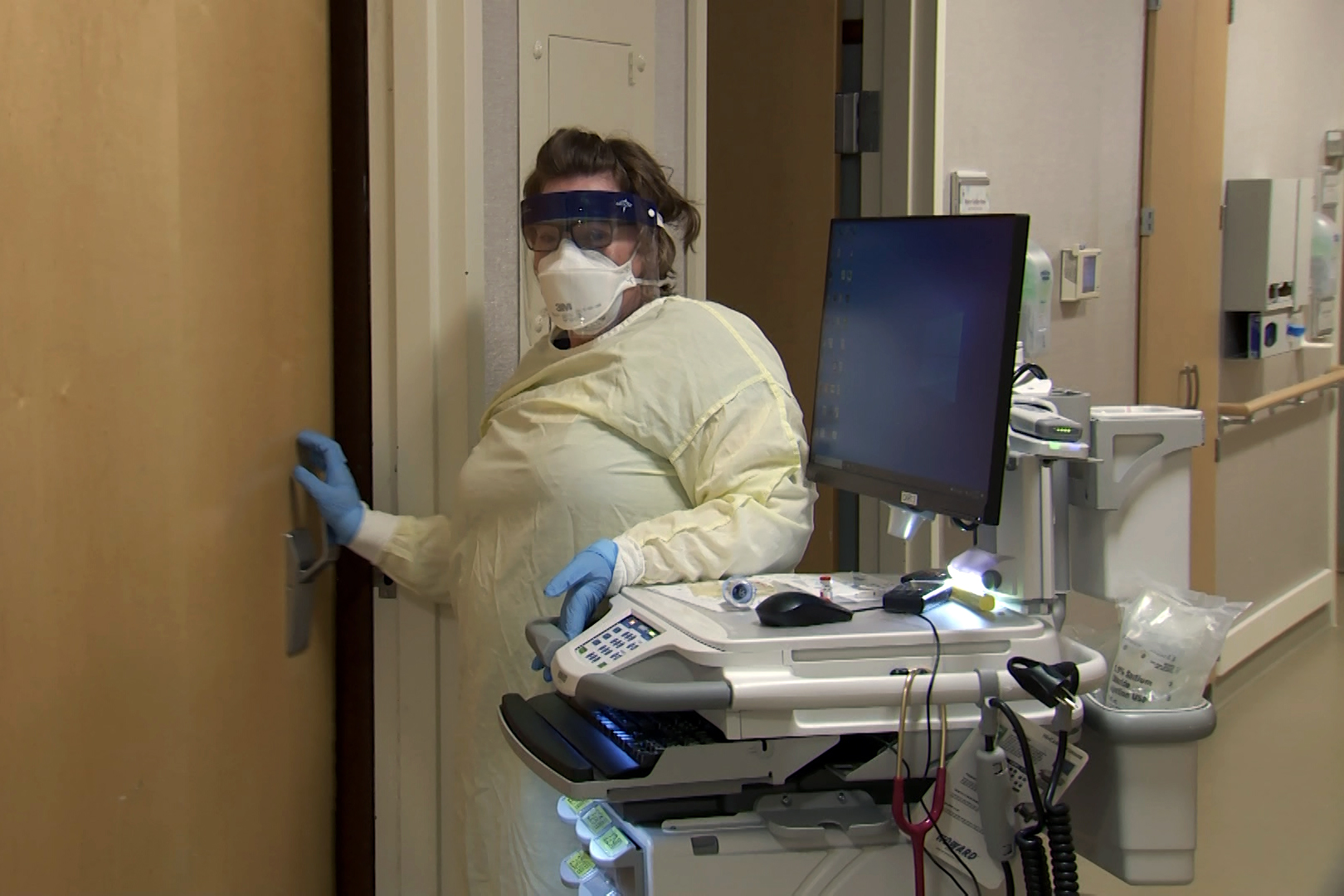
National Guard members are serving in a variety of roles, both clinical and non-clinical, in a number of Indiana hospitals.
(Devan Ridgway, WFIU/WTIU News)
For weeks, hospitals across Indiana have endured a surge of new COVID-19 cases. Once again, the strain has revealed systemic flaws.
An executive order from Gov. Eric Holcomb (R-IN) aimed to assist tired and overwhelmed healthcare workers cope does little to address the problems healthcare experts say will be chronic.
While Holcomb’s executive order greenlighting, the deployment is not new, it allowed for the National Guard’s latest deployment to Indiana hospitals.
Across the state, health systems struggle to retain talent and care for the surge of largely unvaccinated patients sickened by the coronavirus.
“Staffing is an issue for every hospital,” president of the Indiana Hospital Association, Brian Tabor, said.
That’s especially apparent in rural communities.
“Forty percent of all the rural hospitals in Indiana were financially at great risk before the pandemic,” Tabor said. “Where we stand today, I do fear some of those hospitals have been pushed closer to the brink.”
Tabor and other experts say hospitals are spending more to retain and train talent, while many, including the state’s largest health system, IU Health, have cancelled all in-patient procedures.
Full patient rooms and converting ambulance bays into patient triage areas doesn’t translate to more profit.
At Mary Margaret Hospital in Batesville nearly all patient rooms occupied.
Many aren’t vaccinated against COVID-19, and now have the virus. Outside the negative airflow rooms, communities have largely returned to normal, but the healthcare workers and system caring for these patients are at a breaking point.
Rooms with patients suspected of or confirmed with contracting COVID-19 are marked with red placards.
“ISOLATION,” they read. “SEE STAFF BEFORE ENTERING”
Isolation placards line the hallways at Mary Margaret Health in Batesville, IN. (Devan Ridgway, WTIU/WFIU News)
Jamie Schutte, a respiratory therapist at Mary Margaret, has entered these rooms countless times.
“Our workload is quadrupled,” he admits from a med surge room with a COVID patient struggling to fight the virus next door.
In between interviews, a nurse places one of the red placards on the doorframe.It confirms a familiar diagnosis.
As a critical access hospital, during non-emergent times, Mary Margaret cares for up to 25 patients, but today there are nearly that many COVID patients on the floor. That doesn’t include the patients with other conditions requiring hospital stays.
“We are keeping twice and three times the normal number of patients that we are used to seeing,” Devan Royce the Interim Chief Nursing Officer at Mary Margaret said. “Our inpatient volumes been very busy.”
Latest Surge Exposes Systemic Flaws
While the total number of Hoosiers hospitalized with the virus have dropped in recent weeks, local surges continue to overwhelm hospitals.
Schutte is one of a handful of respiratory therapists at Mary Margaret, and has seen a lot over the course of the pandemic.
“What scares me is seeing—since I'm from the community— is seeing family or neighbors, friends that come in and I have to take care of them,” he admits. “In a small community, you kind of know everybody, and [that] makes it hard.”
The problems facing Indiana hospitals aren’t isolated to Mary Margaret. Across the state—and country—healthcare is being pushed to the brink. Experts say unvaccinated COVID patients paired with a number of clinical staffing shortages are testing an already tattered system.
A recent survey places Indiana tied for 49th in the nation on dollars spent per capita on public health. While the state has moved to form a public health commission, decades of neglect cannot be erased overnight.
That lack of spending contributes in a large part, experts say, to why an order from Holcomb—who has joined fellow Republicans in resisting further COVID-19 restrictions—allowed the National Guard to be deployed to several Indiana hospitals.
One of them is Clark Memorial in Jeffersonville.
“It has been a real boost for us to have an extra pair of hands,” Ruth Schmidt, the hospital’s Chief Operating Officer said. “Really what we needed was something, somebody to come in and least give us a couple weeks of an extra pair of hands to help with those things that we want to do, but just haven't had a chance to get to.”
During their deployments, guard members serve a number of varied roles—from COVID testing to patient care and administrative duties.
Members can only be deployed at a hospital for two-week periods. Last week, was their final day at Clark Memorial.
Once the guard leaves, hospitals are forced to resume filling shifts with traveling staff—which come with a high cost—or realigning existing staff.
“We go back to where we were, and we continue on without the help,” Schmidt said. “Which means everybody picks up a little bit more.”
We were supposed to tour the ER as part of our visit, but hospital staff told us it was too crowded. Schmidt and other hospital administrators admit the care patients are receiving is not always to the level they desire.
Inability To Transfer Causes Ripple Effects Systemwide
“To be honest, it does scare me a little,” she admitted. “But I feel like, we are being flexible to make sure we take care of who we can. We make sure that those people we can't take care of we get to an appropriate place that they can get care.”
But the hospitals equipped to provide more intensive care are stretched thin, too.
Many Indianapolis-area hospitals admit they’ve spent significant time on diversion. Diversion temporarily limits or prohibits full hospitals from taking new patients.Hospitals report division time to the state’s Managed Emergency Surge for Healthcare (MESH) coalition.While real time data is hidden due to security concerns, the struggles hospitals face—regardless of size—persists.
A nurse enters a COVID-19 patient's room at Mary Margaret Health in Batesville, IN. (Devan Ridgway, WTIU/WFIU News)
The lack of staff and physical space create ripple effects for small, critical access hospitals like Mary Margaret.
“There's a bottleneck,” Royce said. "It’s the state of Indiana, it's our transferring facilities in Indianapolis and then Cincinnati and not being able to transfer appropriately.”
Royce admits her hospital now keeps sicker patients longer because there is nowhere to transfer them throughout the system.
“That gets scary when you're a critical access hospital and you're trying to figure out how to get patients appropriately, where they need to be,” she said. “The reality is, if there's nowhere for them to go, they're staying here.”
Her frontline staff members experience it daily.
“Normally, we have patients come in and you're with them for two or three days, then go home,” Schutte said. “COVID patients, we're with them every day for a month or better, and then sometimes they don't get to go home. You learn a lot about them before they get too sick to be able to talk.”
Even after 20 months, he admitted it doesn’t get easier.
“You get to know them. It makes it hard,” he said.
While hospitalizations statewide have plateaued, officials remain concerned about future variants, lower than average vaccinations, and the upcoming flu season.
Just over half of eligible Hoosiers have received are fully vaccinated against COVID-19.